Identifying Patterns and Needs for Contraceptive Care Among Men and Women Veterans
Research SummaryPublished Oct 21, 2025
Research SummaryPublished Oct 21, 2025

Photo by Krakenimages.com/Adobe Stock
Practical access to contraceptive care and the ability to choose care that meets one’s needs and preferences is important for an individual’s health and well-being. Although a significant amount of research has been done to examine access to contraceptive care in the United States, particularly among civilian women, there is significantly less understanding about the contraceptive needs, preferences, and experiences of men and women veterans.
Veterans who are eligible for U.S. Veterans Health Administration (VHA) services can access all U.S. Food and Drug Administration–approved contraceptive methods (hormonal and nonhormonal, barrier devices, long-acting reversible contraceptives, sterilization), although some veterans may still incur co-payments for some services, such as for intrauterine device (IUD) insertion, unless exempt. Women veterans often have access to trained women’s health primary care providers (WH-PCPs), although varying levels of services are available on-site depending on the location. In the early 2020s, VHA supported innovative programs intended to improve access to contraception, such as pharmacist-led prescribing, 12-month refills for hormonal contraceptives (the Contraception on Demand program launched in 2021), and an initiative to improve vasectomy access and counseling (the Male Contraceptive Initiative launched in 2023). External veteran-serving organizations (such as the Service Women’s Action Network or Bob Woodruff Foundation) provide a variety of resources to support access to reproductive care for veterans. Regardless of care location, challenges to access and choice can arise from state policy differences, stigma (especially for men), the quality of provider engagement and counseling, and the availability of birth control methods.
RAND researchers conducted a mixed-methods study to identify gaps in contraceptive access and choice among veterans, potential variations in access and choice by such factors as sex and age range, and specific barriers veterans face to accessing their preferred contraceptive methods. The study was sponsored by Arnold Ventures as part of the philanthropy’s portfolio on contraceptive choice and access. Veterans aged 18 to 49 received about a 15-minute web-based survey through two national probability panels (Ipsos’ KnowledgePanel and NORC’s AmeriSpeak) in early 2025. RAND researchers drew items from existing surveys, such as the National Survey for Family Growth (NSFG), to design their survey. The researchers applied weights to the final combined panel sample to ensure representativeness by age, sex, race/ethnicity, region, and other demographics. The team also completed more than 50 in-depth interviews with a sample of survey respondents to explore respondents’ experiences with contraception and potential barriers to access.
This brief details the research team’s findings about veterans’ knowledge of contraception, engagement with providers about contraception, and use patterns of contraception and associated recommendations to improve contraceptive access and choice among veterans of reproductive age.
Some distinguishing characteristics from the nationally representative sample of veterans are as follows:
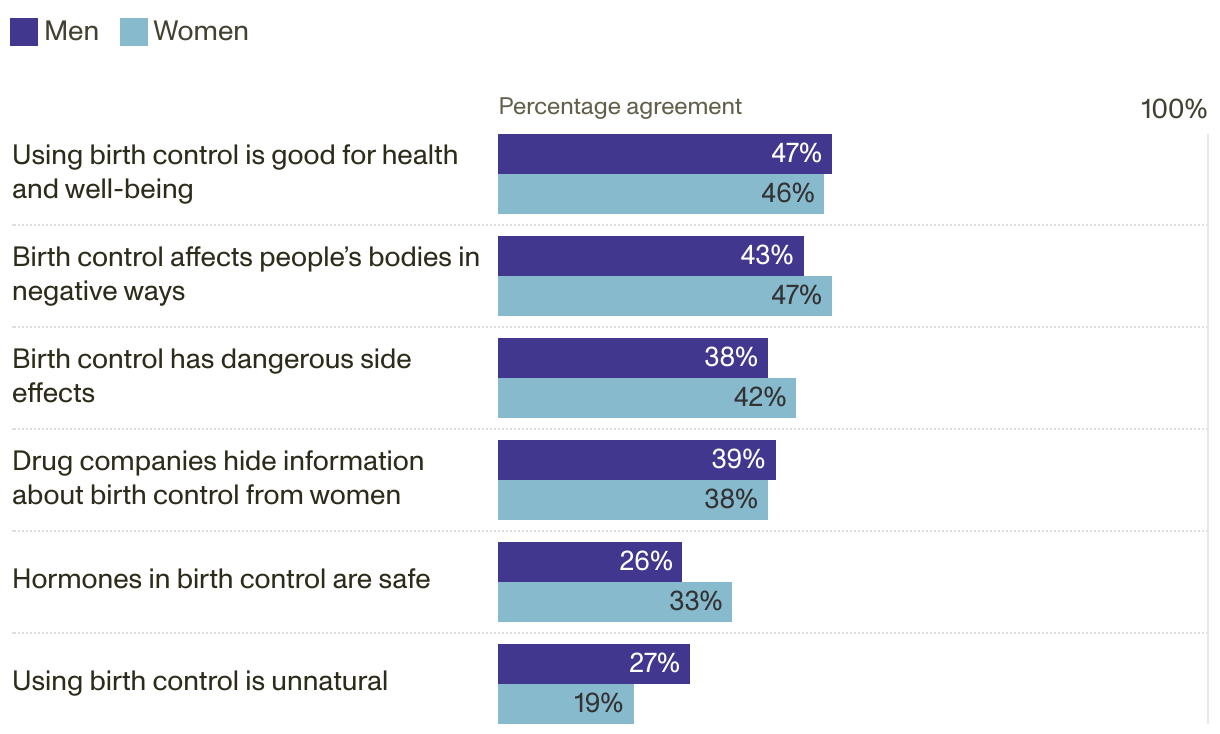
Veterans’ general perceptions of birth control were very mixed (see Figure 1). For example, just under one-half (about 48 percent) of veterans thought that birth control is good for one’s health and well-being, and a similar but slightly smaller proportion (about 44 percent) thought that birth control affected people’s bodies in negative ways. Almost four in ten veterans thought that birth control had dangerous side effects.
From a set of 19 multiple-choice questions on veterans’ knowledge levels about contraception and specific methods, the median score of correct responses was 42 percent; females scored higher than males (58 percent compared with 37 percent), and there were significant differences in more than one-half of the item responses. Veterans had higher levels of knowledge about the ability of condoms to prevent sexually transmitted infections, the ability for semen to be released before ejaculation, and IUDs being less easily noticed by partners. Veterans’ knowledge scores were the lowest about knowing the specific length of time vaginal rings should be kept in place, that emergency contraceptive pills cannot end a pregnancy in its earliest stages, and that women do not need a pelvic exam to receive birth control pills. Finally, veterans were asked about their perceptions of side effect frequency for certain birth control methods. About six in ten had perceptions that were aligned with the side effect frequency reported in the literature. Those with inaccurate perceptions tended to overstate the side effect risks for certain contraceptive methods.
Only 10 percent of veterans reported having a discussion with their providers about birth control in the past year; this was more common among women, with around one in four women having these discussions compared with approximately one in 50 men. Most of these discussions did not take place in VHA health care settings. Despite the lack of conversations about contraception, veterans reported general trust in their providers and high confidence about having productive conversations with their providers about contraception. In interviews, veterans noted that they often initiated discussions about birth control. However, male veterans shared their perceptions that contraception is seen as a female-centric topic that is rarely raised with them by their providers.
To me, it is important that I do feel listened to and that I don’t feel like they’re just trying to push, like, a pill on me.
Female, 40–44, Received contraceptive care at VHA and was sterilized outside VHA more than 12 months ago

Photo by New Africa/Adobe Stock
About one in five veterans used contraception in the past year to prevent pregnancy. The most commonly used methods were condoms, pills, withdrawal, and IUDs. Sterilization rates among veterans were high: 28 percent of men and 38 percent of women reported being sterilized. A little more than one in four men and women reported that they would use a different contraceptive method if it were accessible to them.
Partners played a large role in influencing veterans’ choice of birth control methods, and veterans often came to a joint decision with their partners on which methods would work best and meet their preferences. Male veterans recognized that there are more-limited options for men and stressed the importance of their female partner’s role in decisionmaking about contraceptives. Veterans’ choices of contraception often were tied to their stage of life, with more-permanent contraceptive methods chosen by veterans who no longer wanted to have children.
There were several notable demographic variations in the nationally representative sample of veterans.
Most veterans perceived their post-service contraceptive needs as similar to those of civilians, although some veterans cited certain experiences in the military (e.g., toxic agents, posttraumatic stress disorder, access to sensitive information) as influencing their reproductive choices. Many veterans pointed out gaps in contraceptive information, a lack of proactive discussions with providers, and a general perception that family planning is a “woman’s issue.” Veterans considering sterilization procedures shared their challenges with getting referrals or scheduling appointments, and others shared that counseling about the procedures was inadequate (e.g., a lack of full information about sterilization permanence or failure rates and providers only offering narrow options despite patient interest in alternatives).
I wish that they were a little bit more vocal about it [contraceptives]. . . . But being in the VA system, I know that it’s there. If you asked about it, you want to get educated about it, you can get prescribed it. But I don’t think it’s really just talked about a whole lot. I guess that’s the best way to put it.
Male, 35–39, Received health care at VHA

Photo by Mat Hayward/Adobe Stock
The findings presented in this brief suggest significant education needs for both veterans and providers. Veteran-serving organizations, including VHA, should consider increasing their investment in efforts to address misconceptions and improve veterans’ understanding about family planning needs and methods of birth control.
This study appears to be the first to comprehensively examine contraceptive access and choice among male and female U.S. veterans of reproductive age. Historically, fertility control has predominantly focused on women and often neglected men’s roles and responsibilities in family planning. Men’s perspectives and experiences play a significant role in contraceptive decisionmaking within partnerships. Involving men in these studies can help identify ways to not only improve their own decisionmaking about male-specific contraceptive methods but also identify how they can be more-educated sources of support for female partners. Men’s involvement in these studies would also improve men’s access to and inform their choices about birth control methods more broadly.
Relatedly, the measurement of certain contraceptive constructs, such as contraceptive self-use, tends to be male- or female-focused. The survey discussed in this brief employed neutral wording where possible and a full list of male and female contraceptive methods with questions of use. In addition, some key characteristics to understanding veterans’ experiences involve understanding their locations of care and whether that care is through established referral networks, such as VA community care. However, veterans may not always recognize these terms when reporting about their care. In the analysis stage, RAND researchers learned that there were misinterpretation issues related to these survey items, which suggest a need for more cognitive testing to better measure these constructs and improve survey items.

This publication is part of the RAND research brief series. Research briefs present policy-oriented summaries of individual published, peer-reviewed documents or of a body of published work.
This document and trademark(s) contained herein are protected by law. This representation of RAND intellectual property is provided for noncommercial use only. Unauthorized posting of this publication online is prohibited; linking directly to this product page is encouraged. Permission is required from RAND to reproduce, or reuse in another form, any of its research documents for commercial purposes. For information on reprint and reuse permissions, please visit www.rand.org/pubs/permissions.
RAND is a nonprofit institution that helps improve policy and decisionmaking through research and analysis. RAND's publications do not necessarily reflect the opinions of its research clients and sponsors.
